










“It should be possible to compare this recoil of the blood in the veins to the swelling and turbulence of flooding waters from the rising seas.”
– An early account of venous pulsations in right heart failure by Homberg, Paris, 1704.1
Severe tricuspid regurgitation (TR), which affects 1.6 million people in the US, leads to progressive right ventricular (RV) dilation and failure if left untreated.2,3 However, TR remains undertreated. Most tricuspid valve (TV) surgeries are performed in the context of other planned cardiac surgery and are associated with relatively high morbidity and mortality.4 In this review, we discuss the pathophysiological and epidemiological aspects of TR, and provide a critical overview of the current and future directions of therapy focusing on novel percutaneous approaches.
Tricuspid Valve Complex
The TV complex consists of a fibrous annulus surrounding three leaflets (anterior, posterior and septal) seated between the right atrial and ventricular myocardium.4 The anterior leaflet is generally the largest and most prominent, while the septal leaflet is the smallest and arises medially directly from the tricuspid annulus. The atrioventricular node is adjacent to the base of the septal leaflet.
The TV complex functions as an integral apparatus in coordination with the subvalvular components (consisting of papillary muscles and multiple chordae tendineae). There are two main papillary muscles: anterior and posterior, providing chordae to all three TV leaflets. In contrast, the septal papillary muscle is rudimentary, with chordae tendineae arising directly from the septal wall, resulting in relatively reduced motion of the septal leaflet. This results in the TV behaving partially like a bicuspid valve.5 Additional numerous accessory chordae attach the moderator band to the RV free wall. Together, the bicuspid-like valvular behaviour and the accessory chordal attachments of leaflets form the critical structural basis for the susceptibility of TV to annular dilation and malcoaptation, leading to TR.6
The tricuspid annulus is very elastic and can change markedly by RV preload, afterload, and systolic function. For this reason, the overall volume status and RV function tend to have significant influence on the degree of TR.3
Classification of Tricuspid Regurgitation
Tricuspid regurgitation can be classified into primary, isolated, or secondary causes. Primary TR involves a defect of the valvular apparatus (leaflets, chordae, or papillary muscles).7 There are many aetiologies of primary TR, which include, but are not limited to, congenital heart disease, rheumatic heart disease, myxomatous disease, carcinoid syndrome, infective endocarditis, trauma, radiation and valvular injury as a result of endomyocardial biopsy.8
Isolated TR has been increasingly recognised as an important subtype of TR and is hypothesised to be associated with atrial fibrillation as well as atrial enlargement and dilation.7,9
Secondary TR is by far the most common form of TR in developed nations and occurs as a result of dilation of the RV chamber and/or of the tricuspid annulus, leading to functional regurgitation.10 Various diseases affecting the RV and tricuspid annulus can lead to secondary TR. Common causes of secondary TR are:
- RV remodelling from elevated RV systolic pressure. This can be secondary to left-sided valvular and/or myocardial disease, or secondary to pulmonary hypertension of any cause independent of left-sided cardiac pathology. Rarely, RV dilatation may result from congenital heart disease such as pulmonic stenosis, or from left-to-right shunts (Eisenmenger syndrome) seen in atrial septal defects or anomalous pulmonary venous connections.
- RV remodelling from cardiomyopathy, including ischaemic cardiomyopathy (RV infarction), restrictive cardiomyopathy, or non-ischaemic cardiomyopathy causing RV or tricuspid annular dilatation.
- Atrial-ventricular desynchrony, such as chronic AF or chronic RV pacing causing desynchrony.
- Cardiac implantable leads traversing the TV complex causing TR.
Importantly, secondary or functional TR commonly reflects the presence of, and in turn aggravates, RV failure. Functional TR may diminish or disappear as the RV decreases in size with the treatment of heart failure or atrial-ventricular desynchrony.
Diagnostic Modalities for Tricuspid Regurgitation
The 2020 ACC/AHA guideline for the management of patients with valvular heart disease states that in patients with TR, a transthoracic echocardiogram (TTE) is a class 1 indication for the evaluation of the presence and severity of TR, as well as to determine the possible aetiology for TR, assess RV systolic function, measure the sizes of the right-sided chambers and inferior vena cava, estimate pulmonary artery systolic pressure, and characterise any associated left-sided heart disease. Invasive measurement, as well as right ventriculography, carries a class 2a recommendation and may be useful when clinical and non-invasive data are discordant or inadequate.11
The main goal of TTE is to assess the severity of TR, pulmonary arterial pressure and RV function.12,13 An essential component of evaluation is Doppler echocardiography to identify and quantify the TR jet to help establish and monitor TR severity.14 In patients with TR secondary to dilation of the tricuspid annulus, the right atrium, RV, and tricuspid annulus are all usually dilated.14 The right atrial and RV end-diastolic pressure measurements are often elevated in TR. RV diastolic overload can be detected with paradoxical motion of the septum. In severe TR, systolic flow reversal may be detected in the hepatic vein. TR magnitude on echocardiogram can be determined by the proximal isovelocity surface area method, by quantitative Doppler, and by 3D colour Doppler.15
Notably, assessing the severity of TR can be challenging on echocardiography, and additional modalities, such as CT angiography (CTA) and cardiac magnetic resonance (CMR) may be helpful.14 CMR allows for excellent RV volumetric quantification and calculation of regurgitant volume. Both CMR and CTA can be valuable to help define the geometric relationships between the RV and the tricuspid annulus and leaflets.16
Transoesophageal echocardiography (TOE) can enhance detection of TR, but the estimated severity of TR may be reduced compared to TTE because of sedation during TOE.
Electrocardiography changes are usually nonspecific and variable depending on the cause of TR. Signs of RV failure, such as right bundle branch block, Q waves in V1, and AF and A-V block are commonly found.
Clinical Presentation of Tricuspid Regurgitation
Mild TR is generally well tolerated and asymptomatic in the absence of pulmonary hypertension or right heart failure. As the severity of TR increases, symptoms include signs of right heart failure, including volume overload, fatigue, and dyspnoea. The decline of cardiac output leads to ascites, painful congestive hepatomegaly, and peripheral oedema. In severe TR, patients may exhibit facial vein pulsation, systolic pulsations of the eyeballs, or throbbing pulsations in the neck, which intensify on effort and are caused by severe jugular vein distention.17 In the late stages of TR, weakness, fatigue, and other manifestations of chronic heart failure may dominate, whereas symptoms of pulmonary congestion may become less intense.
In severe TR, elevated right atrial pressure is transmitted to the hepatic veins, which can result in congestive hepatopathy, ascites and massive oedema. Over time, this can lead to hepatocellular dysfunction and eventually cardiogenic hepatic fibrosis or cirrhosis. The development of liver dysfunction in patients with TR can also occur from hepatic ischaemia secondary to decreased cardiac output. Since most cardiac cirrhosis presents in its late stages, correction of TR may not necessarily lead to resolution of liver function abnormalities.18
Cardiorenal syndrome (CRS), defined as the disorders of the heart and kidneys whereby dysfunction of one organ induces dysfunction of the other, has been increasingly recognised as a common consequence of right heart failure.19 Among the five subtypes of CRS, severe TR directly contributes to type 1 (acute) and type 2 (chronic) CRS, which present as acute or chronic decline in kidney function, respectively, as a subsequent event in the setting of initial heart failure.20 The unique impact of RV function on renal haemodynamics in the absence of left ventricular failure has been observed in humans, supported by early experimental models whereby inducing RV failure by graded valvular damage led to a decrease in renal blood flow, preserved estimated glomerular filtration rate (eGFR), and severe salt and water retention, suggesting a unique role of RV in CRS. The significance of TR in causing CRS is further highlighted in a recent study showing that RA/pulmonary capillary wedge pressure ratio, reflecting a disproportionate increase in RV to LV filling pressures, is inversely associated with eGFR in patients with acute heart failure.21–23 Finally, an important observation has been made that hemodynamic metrics reflective of RV function may have prognostic impact on kidney function in heart failure.21
Natural History and Prognosis of Tricuspid Regurgitation
Mild TR has been estimated to be present in about 80% of the population and does not typically confer any negative prognosis. However, moderate to severe TR leads to significant morbidity and mortality.11 Indeed, there has been growing recognition of the prognostic value of the degree of TR as an isolated comorbidity. While the concomitant cardiovascular disease influences survival in patients with TR, increasing severity of TR alone is an independent predictor of mortality, illustrated by several milestone studies.24–30
In a study of 5,223 patients in the US Veterans Health Administration, increasing severity of TR was associated with worse 1-year survival regardless of pulmonary artery systolic pressure or left ventricular ejection fraction.26 Similarly, in a study of 296 patients with TR, those with the highest tercile of quantitative TR measurements had higher rates of death and heart failure, and event-free survival rates decreased among patients with mild, moderate, and severe TR, respectively.27 Even among patients with severe TR, patients with greater TR had worse outcomes and severe TR 1-year mortality rates are reported as high as 45.6%.30,31 Most recently, in a study of patients in the National Echocardiography Database of Australia, which contains 439,558 adults and the largest cohort of TR patients (29%), it was found that after adjustment for clinical factors, increasing grades of TR from mild to severe were associated with increasing risk of all-cause mortality and cardiovascular mortality; even mild TR was an independent predictor of increased mortality in the study.29 Together, these findings highlight the importance of follow-up and early intervention, where possible, in patients with TR.
Tricuspid Regurgitation Therapy: Medical Therapy and Evidence
Medical therapy remains the primary approach for the management of symptomatic TR in most patients. The use of diuretics is the mainstay of therapy for TR and is a class 2a recommendation in the current ACC/AHA guidelines.11 Diuretics improve volume overload and thereby improve symptoms of TR. The current guidelines also recommend treating the primary cause of heart failure (i.e. pulmonary vasodilators to reduce elevated pulmonary artery pressures, guideline-directed medical therapy for heart failure with reduced ejection fraction [HFrEF], of rhythm control for AF) as a class 2a recommendation where TR is thought to be secondary to a primary cause of heart failure.11
Tricuspid Regurgitation Therapy: Surgical Therapy and Evidence
Management of moderate to severe TR may include TV repair or replacement (surgical or transcatheter approach). For patients undergoing left-sided valve surgery with severe TR, concomitant TV surgery is a class 1 recommendation in the current ACC/AHA guidelines.11 However, in symptomatic patients with isolated severe primary or secondary TR, surgery is a class 2a recommendation, under the current valvular heart disease to reduce symptoms and prevent recurrent hospitalisations.11 More recently, the advent of percutaneous options for TR treatment has broadened the treatment possibilities. These are reviewed in a subsequent section of the current paper.
The relative benefit from surgery versus medical therapy remains unclear, and the optimal approach to TR treatment remains debatable, given the scarcity of evidence available concerning long-term outcomes. There is a clear trend towards repair in functional TR surgery, with estimates of nearly 89% of total cases. However, some general conclusions on the prognosis of TR have been made from observational studies. First, the overall rate of surgical treatment for TR is low. In a retrospective analysis of 3,276 patients with isolated severe TR, only a small proportion (5%) of patients with severe TR underwent surgery.32 Second, there is emerging evidence showing greater survival for both primary and secondary TR subgroups undergoing isolated TV surgery (repair or replacement), but it is conflicting.32,33 Moreover, in-hospital mortality for isolated TV surgery is markedly high (8.8%), although outcomes may improve over time. 34–36 To help guide clinical decision-making, a risk score has been proposed to predict surgical risk with isolated TV surgery.37 Third, mortality after TV replacement appears to be significantly higher than that after TV repair, which may reflect selection bias as repair may be reserved for younger and less comorbid patients.34 Finally, there seems to be no difference in survival for patients undergoing surgery compared with medical therapy for patients with isolated severe TR, but a subset of high-risk patients might derive greater benefit from surgery.24,31,32,38
Tricuspid Regurgitation Therapy: Emerging Percutaneous Therapies
Early percutaneous therapy modalities involved placing bioprosthetic valves in the superior and inferior vena cava of patients to treat symptoms associated with TR.39,40 More recently, the advent of TV-specific transcatheter technology has allowed for the expansion of available percutaneous treatment for TR. Most data remains observational with relatively small numbers of patients, but results are promising. The clinical evidence of percutaneous therapies for TR is summarised in Supplementary Material Table 1.
Unique procedural challenges related to percutaneous TR therapy include difficult visualisation of the TV by TOE, as well as the large size of the tricuspid annulus with often a large coaptation gap in severe TR. Moreover, when comparing percutaneous TV therapy, there is no obvious gold standard from a surgical standpoint, and there is no universal consensus as to the best surgical approach (repair versus replacement). To meet some of these unique challenges, multiple transcatheter approaches to address TR and heart failure are currently under investigation or in pilot phases of use, which are reviewed below. The examples of selected devices are shown in Figure 1.
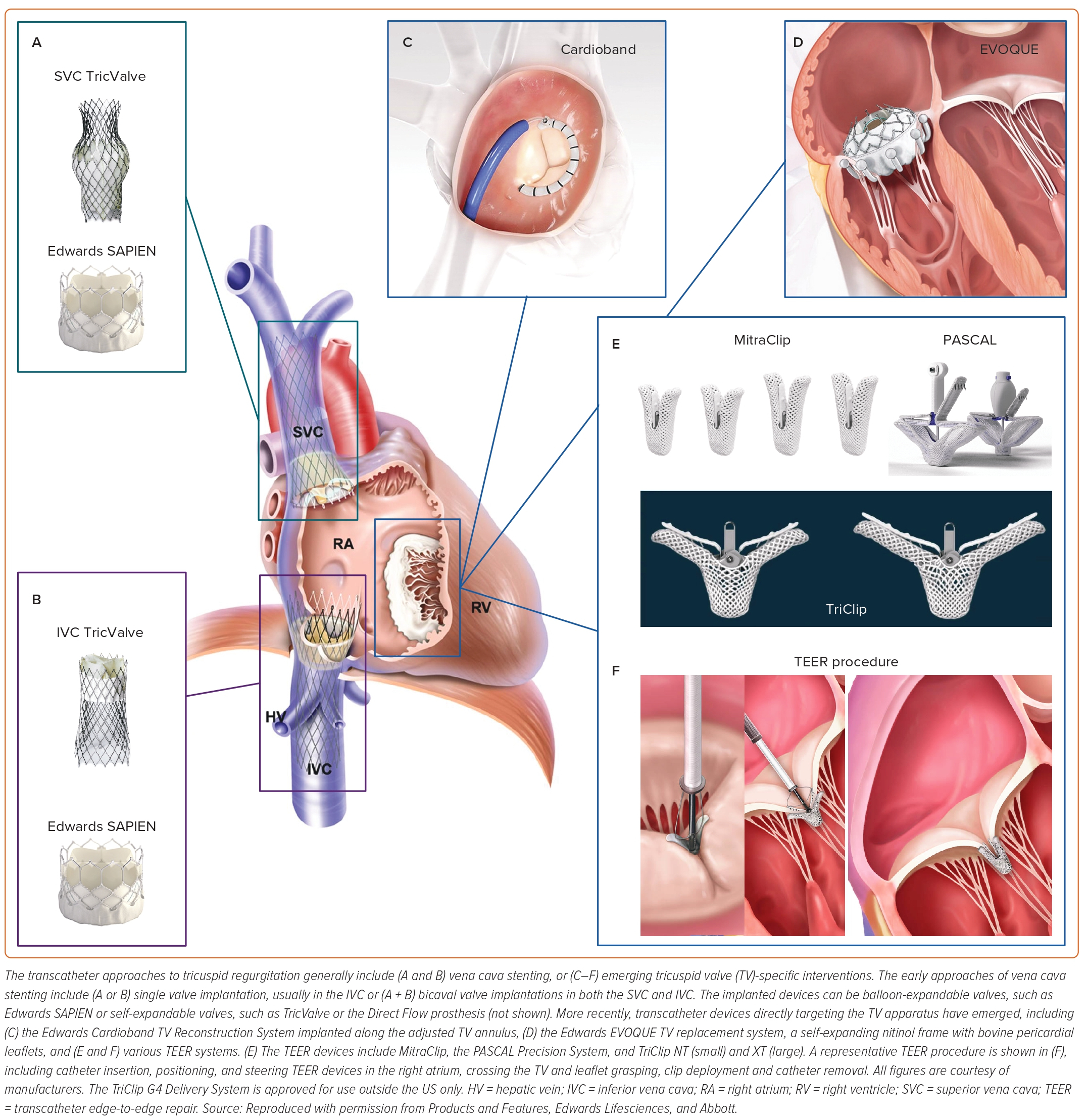
The TriValve Registry reported the outcomes for 472 patients across 22 centres worldwide who underwent transcatheter TV intervention. Propensity-matched results demonstrated that patients undergoing transcatheter tricuspid intervention for moderate or greater TR had greater survival and reduced heart failure hospitalisation when compared with the control group of medical therapy.41,42 Importantly, the transcatheter therapies were varied in this study and included MitraClip (66% of cases), FORMA, Cardioband, TriCinch, Trialign, caval valve implantation, Pascal and NaviGate. Some of these devices are no longer on the market.
The annuloplasty device currently on the market is the Cardioband (Edwards Lifesciences), which is a catheter-delivered annular reduction system that mimics surgical approach.43 The multicentre, prospective TRI-REPAIR study evaluated the results of Cardioband repair in 30 patients with moderate or greater symptomatic functional TR and elevated surgical risk. Follow-up at 2 years demonstrated persistent reduction of septolateral TV annular diameter and in TR grade, and improvements in NYHA class and KCCQ scores.44 The TriBAND study evaluated 61 patients with severe or greater symptomatic functional TR and demonstrated 100% device success, 78% reduction of TR by at least one grade, reduction in TV annular diameter, as well as 1.6% all-cause mortality and improved NYHA class and KCCQ score at 30 days.45 While these results are favourable, the overall patient numbers are small, and further study is needed.
The EVOQUE (Edwards Lifesciences) valve replacement system is the first catheter-based transfemoral system for TV replacement, consisting of a self-expanding nitinol frame, bovine pericardial leaflets and a fabric skirt with nine ventricular anchors. Excellent procedural safety as well as 30-day performance has been demonstrated in a small number of patients treated in first-in-human, compassionate use experience, with durability up to 1 year.46,47 The TRISCEND prospective single-arm trial enrolled 56 patients with symptomatic moderate or greater TR despite medical therapy, with robust reduction in TR.48 Composite major adverse event rate was 26.8% at 30 days largely due to bleeding complications, but also one death and two device embolisation. The ongoing TRISCEND II study will provide more robust data.
Transcatheter edge-to-edge repair (TEER) with the TriClip (Abbott) is based on extensive experience with TEER in the mitral space, with the TriClip device having a similar design to its mitral counterpart, the MitraClip. The TRILUMINATE trial is an international, prospective, single-arm trial investigating the safety and performance of the TriClip in patients with moderate or more TR.49,50 In 86 patients enrolled, 1-year outcomes demonstrated sustained TR reduction, significant reverse right ventricular remodelling, and improved functional status. Overall, major events and all-cause mortality was 7.1% at 1 year.49 The TRILUMINATE pivotal trial, with 700 patients enrolled, is under way.
The PASCAL device (Edwards Lifesciences) is the other TEER device on the market. In the CLASP TR early feasibility study, 34 patients with symptomatic TR despite optimal medical therapy were treated with the PASCAL transcatheter valve repair system.51 The implant rate was 85%, with 52% moderate or less TR, and major adverse event rate of 5.9%. As with other TR reduction techniques, there were significant improvements in NYHA functional class, 6-minute walk ability and KCCQ scores. The CLASP II TR trial results were published at the American College of Cardiology meeting in 2022 and demonstrated favourable results at 1 year with significant improvement in TR, NYHA class and KCCQ score. The PASCAL transcatheter valve repair system has received FDA approval to market in the US on 14 September 2022. The TriClip device is approved for use in Europe but remains investigational in the US.
The clinical benefit of tricuspid TEER compared with medical therapy alone remains uncertain. TRILUMINATE Pivotal is the first international randomised controlled trial to compare TEER with the TriClip transcatheter TV repair system (Abbott) versus medical therapy alone in 350 patients with severe TR.52 The early results favoured the TEER group, with 87% of the patients in the TEER group and 4.8% of those in the control group having moderate or less TR at 30 days. In 1 year, the KCCQ quality of life score changed by a mean ± SD of 12.3 ± 1.8 points in the TEER group versus 0.6 ± 1.8 points in the medical therapy group. TEER was found to be safe, as 98.3% of patients in the TEER group were free from major adverse events at 30 days. The patients enrolled in this trial will be followed for 5 years.
In summary, of the multiple transcatheter approaches to address TV, several relatively small single-armed studies have demonstrated promise for TEER, annuloplasty, and valve replacement with durable results and favourable clinical outcomes at 1 year follow-up. Several randomised controlled trials are currently enrolling patients, randomising them to transcatheter approaches to tricuspid repair or replacement compared with medical therapy, with early results favouring TEER. It remains to be seen what the ideal transcatheter TR therapy approach will be, but given the complexity of TV anatomy, likely the optimal approach will be patient-specific based on anatomic factors. It is likely that within the next few years multiple transcatheter devices will be FDA approved and more widely available for patients with symptomatic TR.
Conclusion
Symptomatic TR, either isolated or in combination with left heart disease, is associated with an unfavourable prognosis. Current medical and surgical treatments may improve symptoms; however, little data exist on long-term survival. Surgical mortality for isolated TV intervention remains elevated and higher than for any other single valve surgery. TV anatomy poses a specific subset of challenges from a percutaneous therapy standpoint, and multiple emerging devices are available to treat TR. To date, several relatively small single-armed studies have demonstrated promise for TEER, annuloplasty, and valve replacement with durable results and favourable clinical outcomes at 1 year of follow-up. Several randomised controlled trials are currently enrolling patients, randomising them to transcatheter approaches to tricuspid repair or replacement versus medical therapy. More data is needed to determine the optimal timing of treatment as well as to establish the appropriate device(s) for each mode of TV failure.
Click here to view Supplementary Material.
Clinical Perspective
- Symptomatic tricuspid regurgitation is associated with significant morbidity and poor prognosis.
- Tricuspid regurgitation remains undertreated, and while current medical and surgical treatments may improve symptoms, little data exists on long-term survival.
- Emerging percutaneous therapeutic modalities for tricuspid regurgitation show promise with favourable clinical outcomes and durable short-term results. However, more study is needed.