










A coronary artery chronic total occlusion (CTO) is defined as a completely occluded coronary artery with Thrombolysis in MI (TIMI) 0 flow (absence of any antegrade flow) and a duration of occlusion of more than 3 months. Approximately 25% of patients with coronary artery disease (CAD) are diagnosed with a coronary CTO on coronary imaging and the incidence of these occlusions rises with the patient’s age.1,2 These lesions consist of an occluded lumen with organised, extensively recanalised thrombus, atheromatous plaque and an adventitia.3 Calcium and lipid components are also found, both intracellularly as well as extracellularly. The occluded lumen is limited proximally and distally by tough collagen-rich fibrous tissue. CTO lesions that are older than 12 months contain tough proximal and distal caps, and the lesions are more calcified, containing less neovascularisation.4 The vascular bed distal to a CTO is perfused by a network of coronary collateral circulation that can maintain adequate perfusion at rest. However, patients can develop symptoms even with well-developed collaterals, especially on exertion when perfusion via collaterals to the affected myocardium is not adequate, resulting in ischaemic myocardial regions.5 Symptoms, and perfusion to these ischaemic regions, can be improved by successful revascularisation by percutaneous coronary intervention (PCI), or bypass surgery in the case of multivessel disease. This can lead to significant improvement in angina and quality of life compared with optimum medical therapy alone.6
CT Coronary Angiography in the Diagnosis of Chronic Total Occlusion
CT coronary angiography (CTCA) is a non-invasive imaging modality that effectively determines the severity and extent of CAD, with the ability to assess plaque morphology, composition and characteristics. When interpreting the CTCA scans, a significant reduction in the size of the lumen that is contrast-filled should be identified.7–9
In the early days, electron beam CT (EBCT) was used to detect the amount of calcification and establish the possibility of coronary disease.10 Technological advancements have led to the development of multi-slice CT (MSCT) with 16, 64 or 128 slices acquired in a single rotation. These scanners have better resolution, fewer artefacts, and the ability to define more anatomical specifications of the coronary arteries and provide detection of morphological characteristics of plaque disease and the stenotic segments. The diagnostic accuracy of CTCA is good compared with invasive coronary angiography, but limitations of excess calcification causing ‘blooming artefact’ and difficulty in visualisation of the lumen still exist.11
CTOs of the coronary vessels on CTCA are a common discovery and diagnosed if there is complete absence of lumen opacification in cross-sectional views. Sometimes retrograde collateral flow of contrast opacifies the lumen distal to the blockage. A CTO can be underdiagnosed on CTCA due to the existence of retrograde collaterals that enable opacification of the artery next to the stenosis. Both total and subtotal occlusions have an interrupted contrast-enhanced lumen on CTCA and, due to the inadequate spatial resolution, it can be difficult to differentiate between the two.12,13
Advances in CTCA technologies have led to better-quality images and lower radiation exposure. Many new CTCA scan readers prefer to use 3D volume rendering (3D-VR) images and software for automatic vessel diameter analysis and vessel segmentation. CTOs can be easily diagnosed using 3D-VR images.14
CT Coronary Angiography in Pre-procedural CTO PCI Planning
The success rate of PCI for CTOs is significantly lower than that for standard PCI. Technological advances and proctoring have improved the success rates among expert operators and centres, but the overall success remains sub-optimal in national registries.15 In the most recent British Society of Intervention Cardiology national audit, a success rate of 74.93% was observed in all CTO PCI patients during 2020–21.16
There remains a need to improve the safety, efficiency and success rate of CTO procedures and CTCA may be a useful tool for this. CTCA can be used in pre-procedural complexity scoring. Conventional fluoroscopic invasive coronary angiography does not always provide the required anatomical details in complex cases.
Different scoring systems are used to assess pre-procedural CTO complexity and facilitate the selection of viable approaches, such as antegrade or retrograde routes, appropriate equipment, and the operator with the greater experience with that particular anatomy. Therefore, these refinements increase the likelihood of success. Primarily, the Japanese CTO registry score (J-CTO) is used, which assigns 1 point for each of the following five features: occlusion length >20 mm, presence of a blunt stump, presence of tortuosity, presence of calcification, and a previous failed attempt.17 The lower the J-CTO score, the higher the anticipated success rate. Other examples of such scores include the Clinical and Lesion (CL) related score by Alessandrino et al. and, recently, the Hybrid Algorithm for Treating Chronic Total Occlusions in Europe, namely The RECHARGE Registry score.18,19
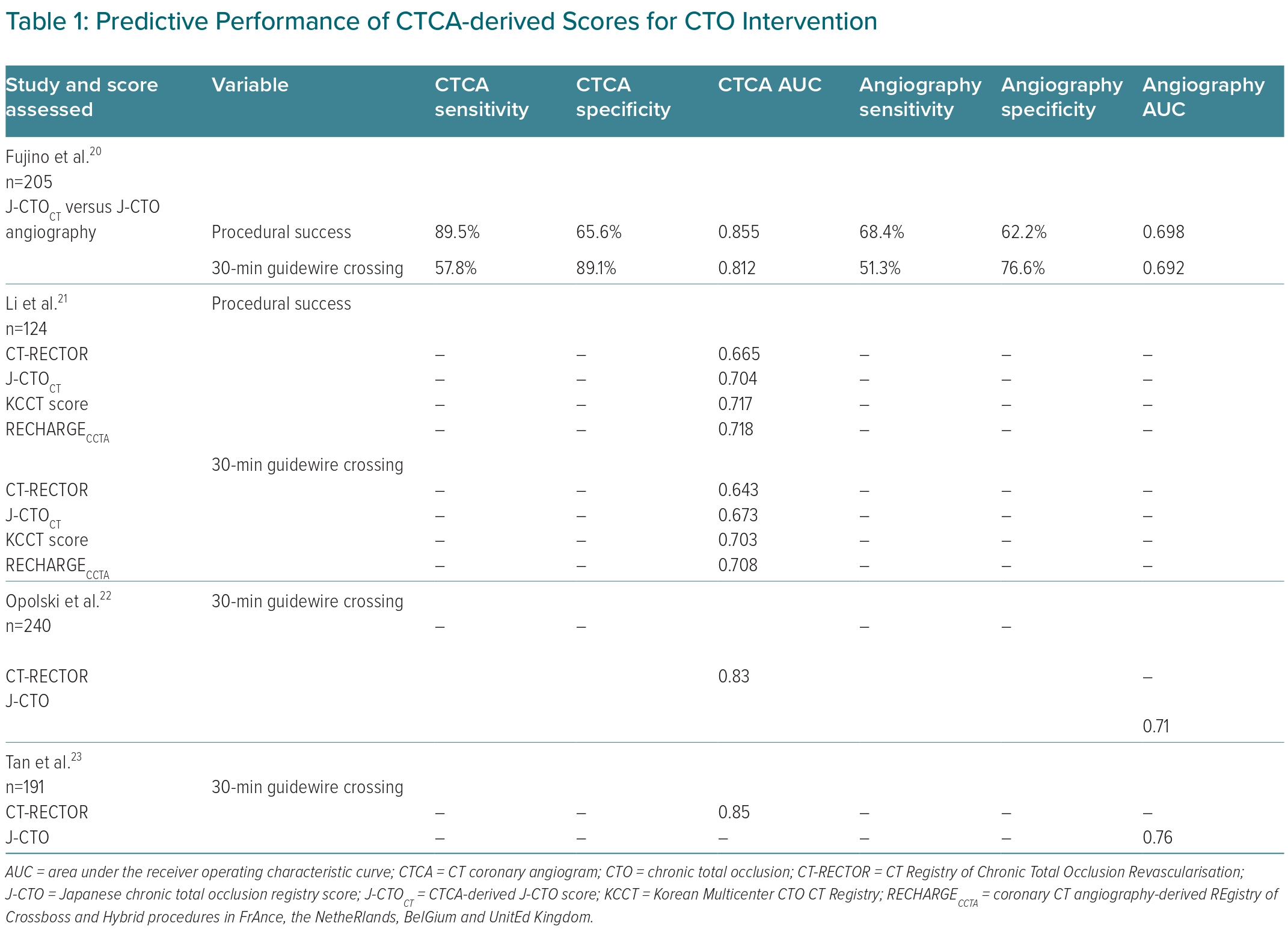
Scoring systems using CTCA have utilised comparisons to data obtained from invasive coronary angiography (Table 1). Fujino et al. studied 205 patients with CTO lesions and pre-procedure CTCA, indicating that a CTCA-driven J-CTO score better predicted potential wire crossing than that of invasive coronary angiogram results.20 A recent study by Li et al. assessed the RECHARGE CTCA scores of 131 patients and compared them with the conventional coronary angiography RECHARGE scores in the prediction of wire crossing and success rate.21 They showed that the RECHARGE CTCA better predicted the success of 30-minute wire crossing. In 2015 Opolski et al. developed the CT-RECTOR scoring system that mainly uses CTCA data.22 That study included 240 participants with consecutive lesions and pre-procedural CTCA, enrolled across four centres. After multivariable analysis, 1 point was assigned for each of the following predictors: severe calcification, multiple occlusions, bending, previously failed PCI, occlusion more than 12 months old, and the presence of a blunt stump. Four different procedural difficulty groups were developed based on the total score, with ≥3 points indicating ‘very difficult’, 2 points indicating ‘difficult’ and 1 point indicating ‘intermediate’, while a score of 0 was regarded as ‘easy’. Thus, the CT-RECTOR score has proven to be more accurate when predicting 30-min wire crossing success compared with the J-CTO score.23
CTCA can also provide detailed anatomical features of the occluded segment. It reliably calculates the length of the occluded segment, which can be difficult in a conventional coronary angiography. It can give details of vessel tortuosity, angles, and the characteristics of the proximal and distal stumps or caps. In addition to the length and the anatomical course of the vessel, CTCA can provide morphological features of the occluded segment and the plaque disease. It can detect and outline the extent of calcification; both are predictors of procedure failure.24 In addition, real-time co-registration with conventional angiographic pictures can guide the CTO operators during the procedure to achieve better outcomes, including presenting the 3D-VR information in the form of angiographic projection that shows the orientation and length of the CTO.
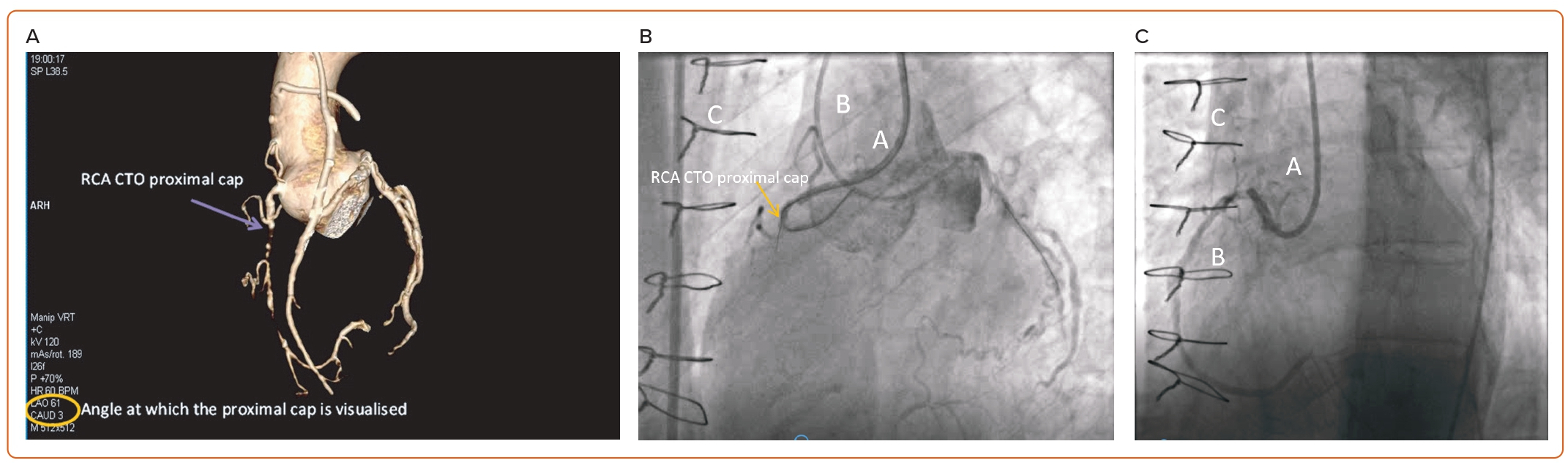
For example, Figure 1 shows a post-coronary artery bypass graft (CABG) patient with an occluded vein graft to his right coronary artery and ongoing angina despite optimal anti-anginal medications who underwent CTCA prior to attempted CTO PCI. The CTCA demonstrated the angle for the proximal cap visualisation, the length of the CTO, presence and extent of calcification and the potential re-entry zone. The CTO PCI was performed using similar angles, which opened up the ambiguous proximal cap, resulting in a successful CTO PCI.
Another advantage of the pre-procedural CTCA is that it can help minimise the amount of contrast used, the radiation dosage and the procedure duration, all of which are important factors in every PCI procedure.25–28 In their randomised control study comparing patients undergoing CTCA or no CTCA prior to CTO PCI, Hong et al. showed that contrast volume was lower in the CTCA group, with no difference in the fluoroscopy time between the two groups (contrast volume: CTCA group, 280 ml versus no CTCA group, 300 ml, p=not significant; fluoroscopy time: CTCA group, 35 min versus no CTCA group, 36 min, p=not significant).29
The Role of CT Coronary Angiography in Post-CTO Intervention
Unsuccessful entry into the proximal cap or unsuccessful re-entry into the distal lumen indicates failure of the CTO PCI. Although unsuccessful, plaque modification and development of new channels may increase the likelihood of further successful intervention.30 For this reason, this initial procedure is commonly called an investment procedure.
CTCA after an investment procedure (failed to re-enter and/or only ballooning of the extra-plaque space) could play an important role in increasing subsequent procedural success by facilitating the detection of details such as the development of new tracks, the direction of the dissection plane, how far the distal entry cap is, and the likelihood of successful antegrade dissection re-entry (by determining the degree of calcification and identifying the area of the artery where this is most likely to be successful).
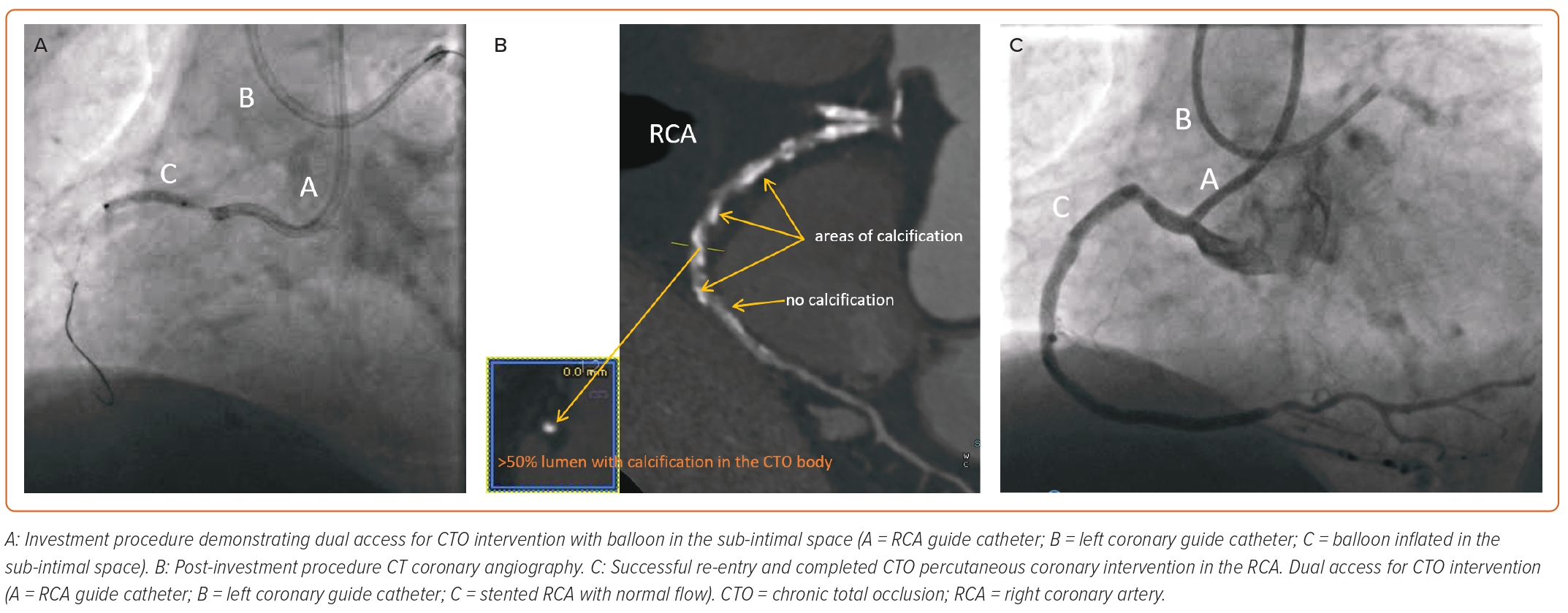
For example, Figure 2 shows a case where the CTO PCI attempt utilised an antegrade dissection re-entry technique in which re-entry into the distal vessel was unsuccessful despite multiple manoeuvres. The sub-intimal tract was ballooned as an investment procedure and the patient underwent outpatient CTCA. This demonstrated heavy calcification in the areas where the re-entry was being attempted. A second attempt at re-entry via the areas that were identified as being free of calcification was successful and the artery was stented. In this case, the CTCA helped in identification of the area where re-entry would be successful.
Another use of post-procedure CTCA is to confirm the success of recanalisation and as a follow-up scan for patients who presented with angina symptoms after previous angiographically successful interventions.
Outcome of CTO Intervention with Prior CTCA Planning
CTO intervention is associated with a higher risk of failure than non-CTO intervention, which has an average estimated success rate of around 70%.31 Although successful CTO intervention is of significant clinical benefit, including improvement of angina symptoms, reduction in the use of medications and reduction in the need for CABG surgery, it is imperative that there is a good clinical indication for proceeding with CTO PCI.32,33 Only then can the optimal clinical risk–benefit–resource usage be justified.
Multiple factors contribute to the increase in the success rate of CTO PCI. Advancements in technology such as wire development, microcatheters, calcium modification technology and the use of intracoronary imaging all play a valuable role. More importantly, however, careful pre-procedural planning, dual injections, the availability of new equipment with specialised wires and support catheters and techniques have all helped increase the success rate.
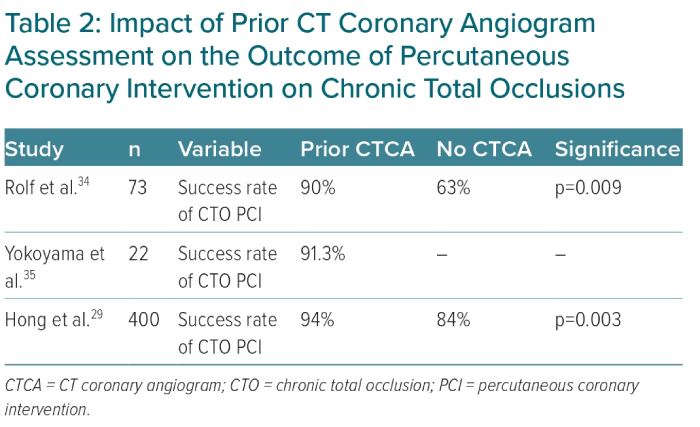
What is the role of CTCA pre-CTO PCI? Different studies have investigated the success rate of CTO PCI after a pre-procedure CTCA (Table 2). Rolf et al. compared 30 patients who had CTCA prior to CTO PCI with 45 patients who did not and found a significant increase in the procedural success rate with CTCA.34 Another study by Yokoyama et al. investigated the use of CTCA prior to CTO intervention and found that CTCA can accurately assess the route of the lesion and provide details on the amount of calcification.35 Both factors resulted in an excellent success rate. Hong et al. conducted the first randomised trial on the use of CTCA in CTO PCI: 400 patients were randomised into either pre-procedural CTCA or no CTCA. A higher success rate was seen in the CTCA group (93.5%) than in the angiography-only group (84%). They also noted fewer immediate complications in the CTCA-guided group. In that study, patients with all J-CTO scores were included, with the average J-CTO score being <2 and successful revascularisation in the CTCA arm was driven by the higher J-CTO (≥2) group.29
Anecdotally, interventional cardiologists limit the use of CTCA routinely in CTO PCI to failed procedures or to patients who have had previous CABG. This could be because one of the limiting factors in the utility of CTCA prior to CTO PCI appears to be the availability of timely scans and/or a paucity of personnel who can explain to the CTO operator the details of the CTO anatomy in a manner that will aid in procedure planning.
Conclusion
CTCA has facilitated the diagnosis of coronary artery disease by enabling accurate assessment of the anatomical features without the need for an invasive procedure.36 It is a rapidly advancing technology with new-generation scanners providing greater resolution, better quality images and lower levels of radiation exposure. CTO is a frequent finding in CT image analysis. Successful revascularisation of CTO with PCI results in improvements in patient outcomes and better left ventricular function while reducing the need for CABG.37
CTCA has its uses during the various steps of CTO PCI, starting from the initial diagnosis, followed by pre-interventional planning, and finally, post-procedure outcome and follow-up. In particular, pre-interventional use has been shown to have a significant impact on the success rate of CTO PCI. Coronary CT can reliably provide details about these anatomical characteristics and hence increase the likelihood of procedural success. The use of the CT-based scoring system in the pre-procedural planning is another useful tool that can help predict the success rate of CTO intervention. All of these features help select the appropriate patient for intervention, aid in planning and help determine the best strategy.
Post-CTO intervention CTCA can be used after an investment procedure to guide further intervention and as a follow-up tool in patients presenting with recurrence of symptoms after previously successful intervention.
New studies, such as CT Coronary Angiography Prior to CTO PCI (NCT05364827), may help identify whether complex CTOs would benefit from pre-procedural CTCA. In this proposed randomised study, patients will be randomly assigned to either CTCA-guided CTO PCI, or direct PCI. The primary endpoint is the success rate in the CTCA arm compared with the non-CTCA arm, while secondary endpoints include the assessment of angina, the need for a repeat procedure, complication rate, procedure length, and wire crossing time. It also aims to provide some health economic and cost-effectiveness data.
Pre-CTO intervention CTCA is a promising technology that appears to predict the success rate of CTO intervention better than the conventional invasive coronary angiography. The rapid advance in technologies and the positive clinical data indicate the usefulness of the routine use of CTCA before CTO intervention to maximise the success rate. Although these data are promising, future large-scale studies are needed to further support these claims. In addition, CTCA (level 2) certification is now more widespread among cardiologists, and this factor may circumvent the limitations mentioned above. The authors concur that the utility of CTCA prior to CTO PCI has the greatest advantage not only in failed procedures and those with prior CABG but also in those with high-score CTOs (e.g. J-CTO ≥2). 