









Nearly every country is now affected by the coronavirus disease 2019 (COVID-19) pandemic. The disease is spreading rapidly and is taxing the global healthcare system, particularly intensive care units (ICUs). Physicians are faced with ethical decisions regarding the allocation of these precious resources, especially ventilators. Although only a few of those infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) require admission to intensive care, the burden on healthcare systems is unprecedented. This article focuses on ethical issues in decision-making regarding COVID-19, particularly in the elderly.
Madrid has been one of the cities with the higher number of COVID-19 cases and casualties so far. We have suffered from limited resources and lived with these ethical issues on a daily basis. Also, Spain is experiencing population ageing at a rate that is unprecedented in Europe and COVID-19 infection is particularly severe in the elderly.1,2
Prioritisation
Prioritisation for the allocation of scarce resources is not confined to the COVID-19 outbreak. Transplant organs are examples of scarce resources where prioritisation criteria for allocation are common and physicians have to make a case-by-case evaluation in order to establish which patient receives the organ. Prioritisation reflects established practices that regulate the distribution of finite resources when demand happens to exceed supply. Discrimination based on sex, race or age has no role in prioritisation unless clearly justified, for example sex mismatch might influence the outcome of a heart transplant.3,4
Prioritisation does not mean that one life is more valuable than another, as all lives are equally valuable. When resources are insufficient to save all those in need, prioritisation means allocating the available assets in the most effective way. This method allows priority treatment of patients more likely to benefit from the scarce resource. Prioritisation should be as objective as possible but also flexible to changes in clinical situation. Transparent mechanisms to determine which patients will receive a specific resource are desirable and should be explained to patients who finally receive an organ, to those who are denied and to the public.
Ageism
Ageism encompasses stereotyping, prejudice and discrimination against people on the basis of their age. Ageism is widespread and an insidious practice that has harmful effects on the health of older adults. A recent systematic review showed that the significant adverse relationship between ageism and health is even more consistent than the relationships found in systematic reviews of the effects of racism on health.5 Moreover, European doctors worry about the care they will receive when they are old, with 80% of healthcare professionals anxious about how they would be treated, suggesting they realise that ageism is very common.6 Paradoxically, increasing numbers of elderly people are remaining healthy and some of them have important international responsibilities. For instance, Pope Francis is now 83 years old and Queen Elizabeth II is 94 (Figure 1).

COVID-19 and the Elderly
The risk posed by COVID-19 is higher for elderly people than for younger people.2 For this reason, medical and political authorities should offer older adults strict preventive measures to minimise the risk of exposure and infection. In the event that an effective vaccine for SARS-CoV-2 is developed, priority should be given to vaccination of the elderly, with the aim of maximising the number of lives saved. This is also true for other preventive measures, such as possible pre- or post-exposure prophylaxis.7
In the case of people with COVID-19, the situation is different. When allocating resources in these scenarios, healthcare professionals might prioritise those most likely to survive over those with remote chances of survival. Making a decision based on chronological age is not justified. In addition to age, other aspects that determine theoretical life expectancy must be taken into account. Biological age and the use of frailty scales and comprehensive geriatric assessment are essential for this purpose. The recent statement of the Executive Board of the European Geriatric Medicine Society insists that advanced age alone should not be a criterion for excluding patients from specialised hospital units.8 If an elderly patient is dismissed from a specialised hospital unit for any reason, access to medical attention, symptomatic treatment and palliative care must be ensured. This last point is essential, as palliative care is frequently suboptimal in elderly patients with other conditions, such as heart failure, and this is probably the case in COVID-19.2,9,10
Therapeutic Adaptation after COVID-19 Admission
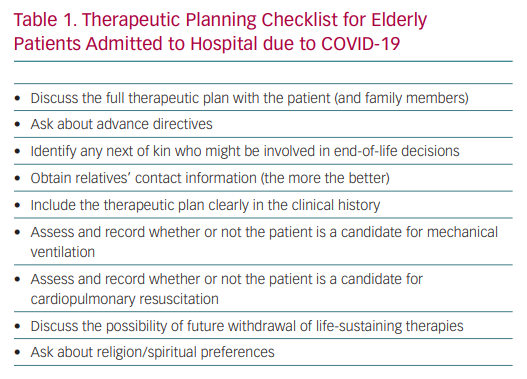
In patients with advanced age who are admitted to hospital due to a severe SARS-CoV-2 infection, it is very important to establish a therapeutic adaptation plan from the time of admission. This plan should be clearly documented in the clinical history, making it clear whether or not the patient is a candidate for mechanical ventilation and, in case of their condition worsening, when to propose the withdrawal of life-sustaining therapies (Table 1). Decisions that maximise survival to hospital discharge, the number of years of life saved and the possibility of living each of the stages of life can be prioritised. In this regard, patients with minimal expected benefit should not be admitted to ICU and the admission of patients with a life expectancy <1–2 years should be carefully evaluated. This applies to patients of all ages. A utilitarian mentality should be applied, which should prevent prejudice against the elderly. For example, a frail elderly patient might have a low chance of surviving the prolonged intubation required to recover from COVID-19 pneumonia, but this is also the case for young patients with severe comorbidities.11
The Madrid Experience
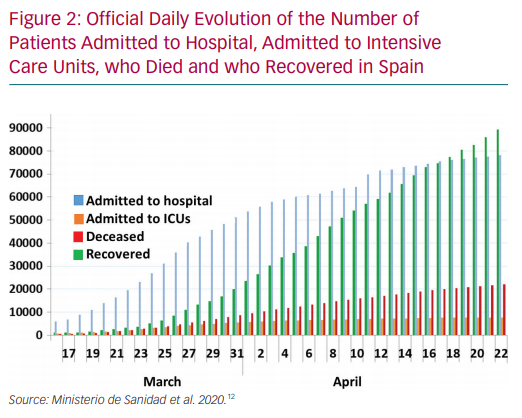
During the peak of the outbreak, more than two-thirds of beds in most hospitals in Madrid were occupied by patients with COVID-19. Figure 2 depicts the official numbers of patients admitted to hospital, admitted to ICUs, who died and who recovered in Spain between mid-March and the middle of April.12 Non-invasive ventilation was attempted frequently, even using improvised alternative strategies like the modified Easybreath diving mask to administer continuous positive airway pressure therapy. Invasive ventilation was often necessary and, in spite of tremendous efforts by the hospitals (for example Gregorio Marañón University Hospital opened ICUs in operating rooms and in the library), there were not enough ICU beds for all the critically ill patients who needed them. The limited availability of ventilation support was even more problematic due to the prolonged intubation – often more than 3 weeks – that many of these patients required. The news that prioritisation criteria were being applied in Spanish hospitals sparked widespread controversy and triggered a debate about the right of every individual, particularly the elderly, to access specialised healthcare.13
Use of Off-label Therapies
Effective therapies for this novel coronavirus are needed urgently and several clinical trials are now underway.14 Meanwhile, the use of use of off-label therapies based on in vitro data and early clinical experience with COVID-19 has increased dramatically; examples include remdesivir, lopinavir, ritonavir, interferon, chloroquine, hydroxychloroquine, azithromycin, tocilizumab, steroids and cyclosporine. To date, no therapies have been shown to be effective.15 Moreover, some of these drugs have frequent and potentially life-threatening side-effects, particularly in the elderly. Most are known to prolong the QT interval and can have a proarrhythmic effect.16
Confinement: Pros and Cons
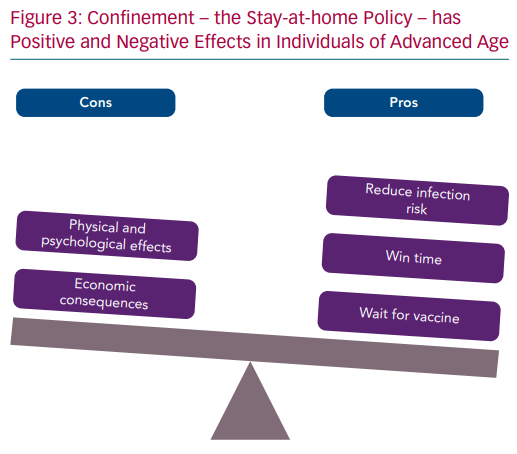
Confinement is an effective way to decrease SARS-CoV-2 transmission and is a way to win time until effective therapies are developed and/or an effective and safe vaccine is available. However, the stay-at-home policy has negative effects in those with advanced age (Figure 3). The psychological risk of confinement is particularly high among vulnerable populations, such as those in a situation of dependence or that live alone. The negative consequences are multifaceted, with physical, mental and social aspects. Staying at home for long periods of time facilitates sedentary behaviours and might worsen previous frailty or pre-frail conditions. At the time of writing this article, our parents/grandparents (aged 82 and 78) have not left their home for 2 months. We are certainly concerned about their situation. Moreover, confinement is extremely negative for the economy and the elderly might end up suffering the consequences of a severe economic depression. Finally, the legal situation varies a lot from country to country. New laws have created legal frameworks that frequently restrict or prohibit the movement of people and vehicles. Some countries have severe penalties for those who do not comply with the new rules.
Family and Mourning
The COVID-19 pandemic has isolated the elderly not only at home but also in hospitals. Visits are usually not permitted. Several patients of advanced age with severe infection have died alone in the hospital or in nursing homes.
The suffering of the family does not end there, as containment measures also apply in the context of mourning, which adds trauma to that of death itself. Corpses are considered potentially infectious, so are deposited as soon as possible in a body bag that will never be reopened. During the peak of the outbreak in Madrid, we had so many deaths that an ice rink had to be used as a provisional morgue. It was frequently impossible for families to see their deceased loved ones one last time.
The rules of social distancing put in place by the health authorities applies also at funerals. Services must be limited to close family members only (with a maximum of three people), usually with video recording and streaming for those who wish to attend the funeral from a distance. Finally, the vast majority of older people in Spain are Catholic. The fact that public masses have been cancelled makes the situation even more difficult for families.
Conclusion
COVID-19 in elderly patients raises some ethical issues; however, most of these issues are similar to ethical problems in other conditions, such as heart failure.17–19 The correct prioritisation for the allocation of scarce resources should be based on various factors relating to the individual. Chronological age should not be the only factor that influences the decision-making process. This is essential to good clinical practice.
{kind=link}