










Obstructive sleep apnoea (OSA) is strongly associated with cardiovascular disease (CVD).1 A few studies in Asia have reported an OSA prevalence ranging from 4.1% to 7.5% in men and from 2.1% to 4.5% in women, with an overall prevalence of 8.5% in the general adult population aged >18 years.2,3 Furthermore, a multi-ethnic southeast Asian country has shown an increase in prevalence to 30%.4 The influence of ethnicity on prevalence has also been demonstrated.4,5
The reported prevalence rates of OSA in patients with coronary heart disease, stroke, heart failure (HF) and arrhythmia are as high as 65%, 75%, 55% and 50%, respectively.6–10 In studies on Asian patients with coronary artery disease undergoing percutaneous coronary intervention or surgical revascularisation, the prevalence of OSA is around 45–50%.11,12 However, the prevalence of OSA among Asian patients with other forms of CVD is less well established.
Given the limited published clinical evidence and country-specific guidelines on the management of OSA in patients with CVD in the Asia-Pacific region, the Asian Pacific Society of Cardiology (APSC) developed consensus recommendations to guide general cardiologists, internal medicine specialists practicing cardiology and sleep physicians in the Asia-Pacific region on the diagnosis and treatment of OSA in patients with CVD. These recommendations are intended to improve screening, early diagnosis and treatment throughout the Asia-Pacific region.
Methods
The APSC convened an expert consensus panel to review the literature on the screening, assessment and treatment of OSA, discuss gaps in current management, determine areas where further guidance is needed and develop consensus recommendations on the diagnosis and management of OSA in patients with CVD. The 16 panel experts were members of the APSC who were nominated by national societies and endorsed by the APSC’s consensus board or invited international experts. The expert consensus panel comprised cardiologists and sleep specialists from Japan, Myanmar, Singapore, Taiwan, Thailand and Vietnam.
After a comprehensive literature search, applicable articles were reviewed and appraised using the Grading of Recommendations Assessment, Development, and Evaluation system, as follows:
- High (authors have high confidence that the true effect is similar to the estimated effect.
- Moderate (authors believe that the true effect is probably close to the estimated effect).
- Low (true effect might be markedly different from the estimated effect).
- Very low (true effect is probably markedly different from the estimated effect).13
Using these levels of evidence, the authors adjusted the level of evidence if the estimated effect when applied to the Asia-Pacific region might differ from the published evidence because of various factors such as ethnicity, cultural differences and/or healthcare systems and resources.
The available evidence was then discussed during a consensus meeting held in April 2021. Consensus recommendations were developed during the meeting, which were then put to an online vote. Each recommendation was voted on by each panel member using a three-point scale (agree, neutral, or disagree). Consensus was reached when 80% of votes for a given recommendation were agree or neutral. In the case of non-consensus, the recommendations were further discussed via email and revised accordingly until the criteria for consensus were fulfilled.
Consensus Recommendations
Screening and Diagnosis
Recommendation 1. Any one of the following conditions should prompt the clinician to screen patients for OSA:
- hypertension;
- type 2 diabetes;
- obesity;
- coronary artery disease;
- stroke;
- HF; or
- arrhythmia.
Level of evidence: Very low.
Level of consensus: 81.25% agree; 12.5% neutral; 6.25% disagree.
Recommendation 2. Symptoms of OSA or screening questionnaires, such as STOP-Bang, may be used to screen for OSA in patients with CVD.
Level of evidence: Low.
Level of consensus: 87.5% agree; 12.5% neutral; 0% disagree.
Recommendation 3. Patients with the following conditions should be referred to a sleep specialist for sleep testing:
- resistant hypertension;
- AF requiring cardioversion/ablation; or
- unexplained pulmonary hypertension.
Level of evidence: Moderate.
Level of consensus: 100% agree; 0% neutral; 0% disagree.
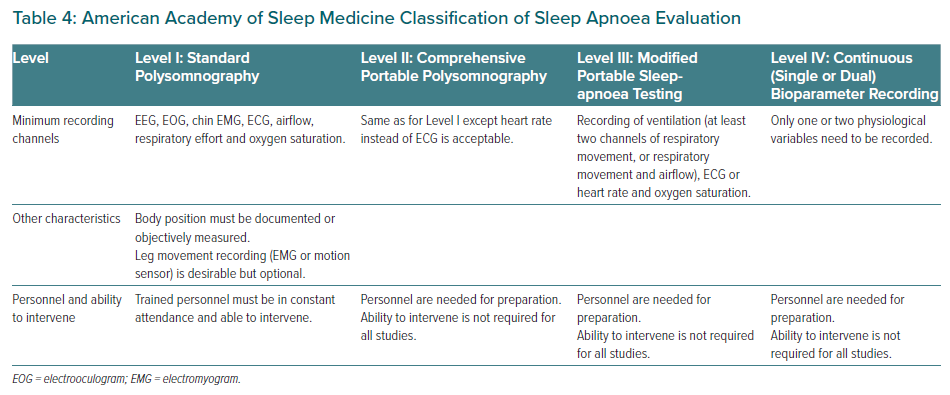
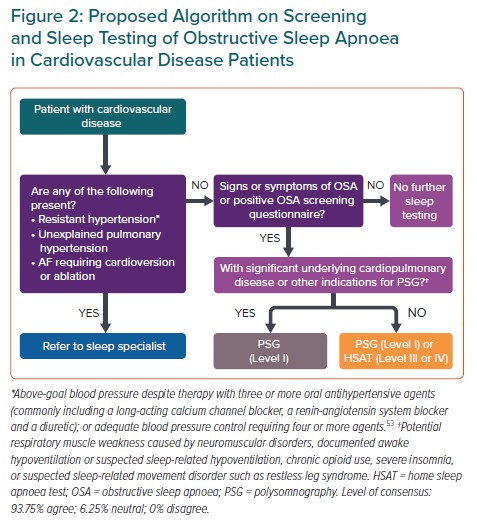
Recommendation 4. In patients suspected of OSA after screening with significant cardiopulmonary disease (HF, congenital heart disease or complicated valvular disease), polysomnography (Level I) should be used to diagnose OSA. Level III or Level IV sleep studies should not be used to diagnose OSA in these patients because of the complexity of the clinical scenario, which may lead to misdiagnosis.
Level of evidence: Very low.
Level of consensus: 87.5% agree; 12.5% neutral; 0% disagree.
Recommendation 5. In patients with a high pre-test probability of moderate to severe OSA without significant cardiopulmonary disease or stroke, home sleep apnoea testing (Level III or IV) or polysomnography (Level I/II) may be used to diagnose OSA.
Level of evidence: Moderate.
Level of consensus: 93.75% agree; 0% neutral; 6.25% disagree.
Recommendation 6. Sleep studies conducted on patients with CVD should be scored and reported by an adequately trained sleep specialist.
Level of evidence: Very low.
Level of consensus: 87.5% agree; 12.5% neutral; 0% disagree.
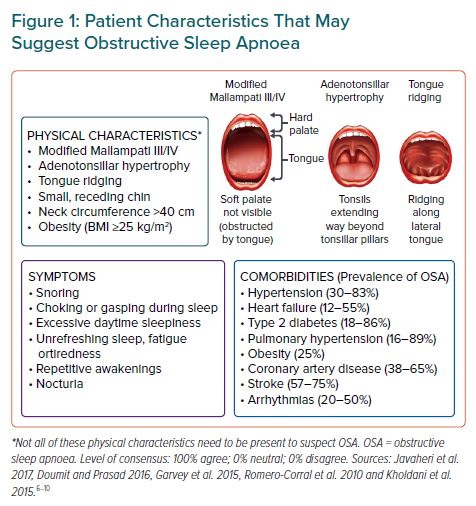
Because of the association between OSA and CVD, it is not surprising that patients with certain CVDs and/or cardiovascular risk factors have a disproportionately high prevalence of OSA (Figure 1).6–10 Hence, the panel voted to screen patients with these conditions, namely hypertension, type 2 diabetes, obesity, coronary artery disease, stroke, HF and arrhythmia. This recommendation is in line with the 2009 recommendations from the Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine (AASM).14 Certain physical features should also prompt physicians to screen for OSA (Figure 1). It should be noted that the Asia-Pacific classification of BMI has a lower cut-off value for the obesity category (25 kg/m2) than the WHO’s classification (30 kg/m2).15
However, some expert panel members noted that screening patients with these fairly prevalent conditions may lead to cardiologists needing to screen a high proportion of patients in daily practice. Others noted that the benefit of screening varies across the conditions, with some conditions, such as hypertension, obesity, coronary artery disease, HF and AF (rather than other arrhythmias), having stronger evidence of benefit.
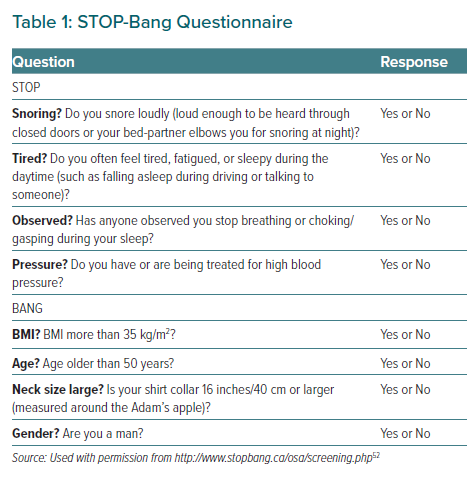
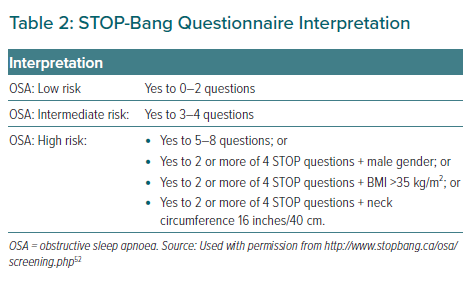
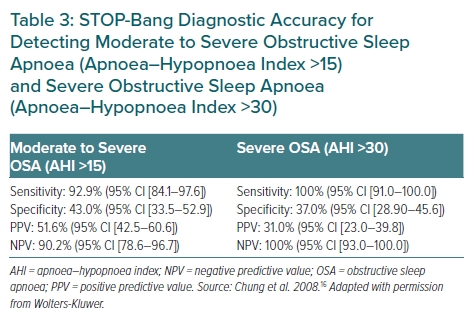
A number of screening questionnaires are available that can be used to screen patients for OSA. During the expert panel meeting, most of the panellists reported that STOP-Bang is one of the most commonly used questionnaires at their respective institutions, largely because of its ease of administration compared with other questionnaires, such as the Berlin questionnaire (Tables 1, 2 and 3).16 STOP-Bang was also shown to have the best diagnostic accuracy for OSA.17
A study conducted on a multi-ethnic Asian population also concluded that the STOP-Bang questionnaire could be used as a screening tool among Asians in view of its moderate sensitivity and high negative predictive value for patients with moderate-to-severe OSA and severe OSA.18
The benefit of interventions in patients without OSA symptoms, such as excessive daytime sleepiness, remains unclear. A rapid and easy-to-perform screening test is needed; thus, the panellists also voted that checking for symptoms of OSA is a reasonable screening tool for daily practice (Figure 1).
Patients with resistant hypertension, AF requiring cardioversion/ablation, or unexplained pulmonary hypertension have an exceptionally high risk of severe cardiovascular adverse events. In these patients, treatment for OSA, if present, has been shown to confer benefit.19–23 Hence, the panel voted in favour of early referral to a sleep specialist for prompt evaluation in such patients. Several panellists also noted that after thorough evaluation, sleep specialists may be able to identify underlying causes of these conditions without needing to proceed to sleep testing or to identify patients who would not benefit from further sleep testing.
The 2020 European Society of Cardiology guidelines on the management of AF recommended that OSA treatment should be optimised to reduce AF recurrences and improve AF treatment results, with a Class IIB recommendation (level of evidence C), and stated: “It remains unclear how and when to test for OSA and implement OSA management in the standard work-up of AF patients.”24 In the multidisciplinary clinical management strategy proposed by Tietjens et al., diagnostic sleep testing for all patients with recurrent AF following either cardioversion or ablation, including those without symptoms of sleep-disordered breathing (SDB), as well as AF patients who are persistently symptomatic, challenging to pharmacologically rate control or managed via rhythm control strategies, when there is a suspicion for sleep apnoea based on comprehensive sleep assessment.19
The APSC consensus agrees with these recommendations and acknowledged the importance of an accurate diagnosis in these patients. Hence, the panel voted in favour of an early referral to a sleep specialist for all AF patients requiring cardioversion or ablation (e.g. those persistently symptomatic despite initial rate/rhythm control strategies), regardless of the presence of clinically suspected SDB.
Patients with significant cardiopulmonary disease (HF with reduced ejection fraction, congenital heart disease or complicated valvular disease) are at a high risk of central sleep apnoea (CSA) or mixed sleep apnoea.6,25 Polysomnography (Level I) rather than home sleep apnoea testing (HSAT) should be the diagnostic test of choice if patients have coexisting and significant cardiopulmonary disease, a history of stroke, or suspected non-respiratory sleep disorders (Table 4). This recommendation is in line with AASM and American Heart Association (AHA)/American College of Cardiology (ACC) guidelines.18,26 Other conditions that may affect the accuracy of HSAT include potential respiratory muscle weakness due to neuromuscular conditions, chronic opiate use and environmental or personal factors that may interfere with the conduct and interpretation of HSAT.26
In contrast, among patients with a high pre-test probability of moderate to severe OSA (including those with very severe OSA) after screening but without significant cardiopulmonary disease or stroke, both HSAT (Level III or IV) and polysomnography (Level I) may be used to diagnose OSA.27,28 In this context, clinicians may use the AASM definition of high pre-test probability of moderate to severe OSA, which includes patients with daytime hypersomnolence and at least two of the following: habitual loud snoring, witnessed apnoea or gasping/choking, or diagnosed hypertension.26
Finally, because of the complexity of interpreting sleep studies, such tests conducted on patients with CVD should be scored and reported by a qualified or adequately trained sleep specialist.29 The expert panel also reported that at some centres in the region, sleep tests are scored by a registered sleep technologist and interpreted by a sleep specialist.
Figure 2 summarises the screening and testing pathway for patients with CVD. However, one panellist cautioned that some patients with HF may require further sleep testing, even with a negative OSA screening questionnaire or in the absence of signs and symptoms of OSA.
Treatment and Referral
Recommendation 7. All patients undergoing OSA treatment should also undergo lifestyle modification and educational and behavioural interventions for OSA, as well as for weight loss if they are classified as overweight or obese.
Level of evidence: Very low.
Level of consensus: 100% agree; 0% neutral; 0% disagree.
Recommendation 8. OSA treatment improves daytime sleepiness and cognitive function. In observational studies, continuous positive airway pressure (CPAP) therapy for OSA is strongly associated with reduced rates of adverse cardiovascular events, but randomised control trial evidence to support CPAP therapy in non-sleepy OSA patients with CVD is inconclusive.
Level of evidence: Low.
Level of consensus: 93.75% agree; 6.25% neutral; 0% disagree.
Recommendation 9. Patients with HF and OSA may undergo CPAP therapy, which has been shown to improve ventricular function, symptoms and quality of life.
Level of evidence: Moderate.
Level of consensus: 93.75% agree; 6.25% neutral; 0% disagree.
Recommendation 10. Patients undergoing rhythm control for AF who have moderate to severe OSA should undergo CPAP therapy to reduce the risk of AF recurrence.
Level of evidence: Low.
Level of consensus: 93.75% agree; 6.25% neutral; 0% disagree.
Recommendation 11. Patients with CVD and OSA whose OSA symptoms persist despite treatment or who are non-adherent to OSA therapy should be reviewed by a sleep specialist.
Level of evidence: Very low.
Level of consensus: 100% agree; 0% neutral; 0% disagree.
All patients with CVD and OSA should be educated with regard to their diagnosis, risk factors and the natural history and consequences of OSA.15,30 They should also be educated on the impact of their treatment and encouraged to continue treatment. Furthermore, all patients should be educated on lifestyle modifications, sleep hygiene and behavioural interventions that may help to minimise the impact of OSA. These include interventions to help reduce weight in patients who are classified as overweight or obese; improved sleep positions in cases of positional OSA; and the avoidance of alcohol and medications that may worsen OSA (e.g. benzodiazepines, barbiturates, other anti-epileptic drugs, sedative antidepressants, antihistamines and opiates). When such medications are necessary, their use should be closely monitored and the dose carefully titrated, if possible.
Weight loss and exercise should be recommended to all patients with OSA who are classified as overweight or obese.14,30–35 Weight loss has been shown to improve overall health and metabolic parameters, decrease the apnoea–hypopnoea index (AHI), reduce blood pressure and improve quality of life for patients with OSA, although weight loss alone rarely leads to complete remission of OSA. Given that obesity and inactivity are cardiovascular risk factors, weight loss and exercise are also recommended in patients with CVD and OSA. Exercise may also modestly improve OSA, even in the absence of significant weight loss. A 2014 meta-analysis found that a supervised exercise program significantly improved AHI (mean change, −6 events/hour), sleep efficiency, subjective sleepiness and cardiorespiratory fitness, even without substantial weight loss.36
In a randomised clinical trial (RCT), 2,717 adults aged between 45 and 75 years with moderate to severe OSA and coronary or cerebrovascular disease were randomised to undergo CPAP plus usual care or usual care alone. The study found that the primary composite endpoint of death from cardiovascular causes, MI, stroke, hospitalisation for unstable angina, HF, or transient ischemic attack was not significantly reduced by CPAP therapy. However, CPAP therapy significantly reduced daytime sleepiness (p<0.001) and significantly improved the physical and mental subscales of the 36-Item Short Form Health Survey of the Medical Outcomes Study.37 It should be noted that this study excluded patients with severe daytime sleepiness (Epworth Sleepiness Scale score of >15), although these patients are most likely to benefit from CPAP therapy.
Some observational studies have suggested that CPAP therapy may be effective in reducing cardiovascular outcomes (e.g. all-cause mortality, cardiovascular mortality, MI, stroke, repeat revascularisation) in patients with coronary artery disease, including after percutaneous coronary intervention.38–41 However, this benefit has not been confirmed in RCTs. A meta-analysis of nine RCTs (n=3,314) on adult patients with polysomnography-diagnosed OSA and any CVD found that the primary outcomes (i.e. all-cause death, cardiovascular death, acute MI, stroke and any major cardiovascular event) were not significantly reduced in patients undergoing CPAP therapy (pooled RR 0.93; 95% CI [0.70–1.24]; I2 49%).42 Possible reasons for this lack of benefit in the primary outcome include the overall low adherence to CPAP therapy, the inclusion of patients with low levels of symptoms or a heterogeneous pool of patients with different disease phenotypes and arterial oxygen desaturation and the potential lack of efficacy of CPAP in reducing recurrent cardiovascular events in patients with advanced or symptomatic atherosclerotic vascular disease.43–45
The 2017 AHA/ACC guidelines on HF identified CPAP therapy as a reasonable treatment strategy (class IIb) to improve sleep quality and daytime sleepiness in patients with CVD and OSA.46 Furthermore, CPAP therapy has beneficial haemodynamic effects, such as diminished systemic venous return, right ventricular preload and left ventricular afterload, as well as improved pulmonary total vascular resistance and ventricular diastolic function.47,48
Patients with paroxysmal AF, including those undergoing rhythm control strategies, such as cardioversion or ablation and moderate to severe OSA should undergo CPAP therapy to reduce the risk of recurrence. Multiple observational studies have assessed the ability of CPAP therapy to reduce the AF burden after ablation or cardioversion. Although limited by methodological issues and small sample sizes, these studies largely support the use of CPAP therapy in reducing the burden of AF.49 Furthermore, data from 1,841 patients with OSA and AF in the ORBIT-AF registry showed that patients who undergo CPAP therapy are less likely to progress to more permanent forms of AF than patients who do not undergo CPAP therapy (p=0.021).50
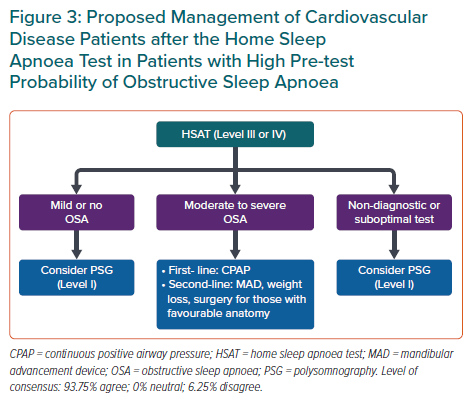
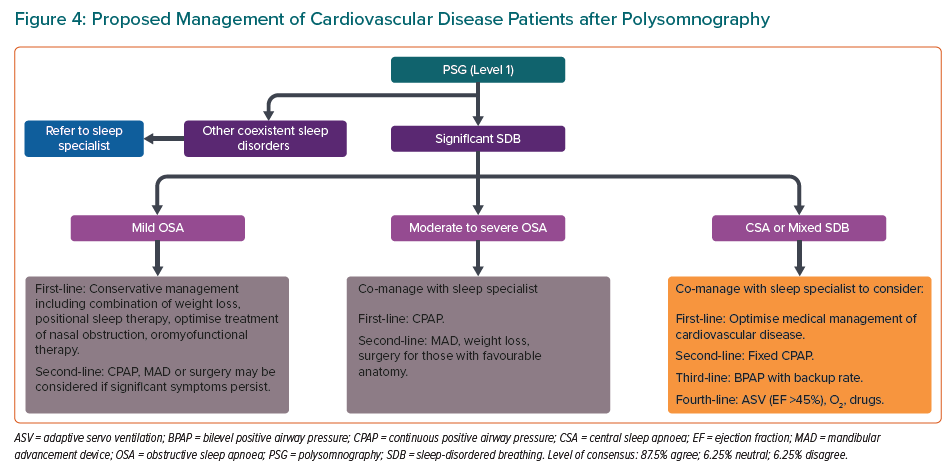
The proposed management of patients with CVD after HSAT in patients with a high pre-test probability is outlined in Figure 3. Figure 4 shows the proposed management of patients with CVD after polysomnography. In this algorithm, the first-line treatment for mild OSA is conservative management, which includes a combination of weight loss, positional sleep therapy, optimised treatment for nasal obstruction and oromyofunctional therapy. One panellist noted that oromyofunctional therapy requires adequate training of healthcare professionals, which may limit its implementation in some areas of the Asia-Pacific region. Some expert panel members emphasised that co-management with a sleep specialist is encouraged in patients with moderate to severe OSA, or for patients with mild OSA if the attending cardiologist has inadequate expertise in its treatment. They also noted that a referral to an otorhinolaryngologist or dental sleep specialist for alternative OSA therapies may be needed in some patients with moderate to severe OSA. Finally, they emphasised the complexity of treating patients with CSA or mixed SDB; hence, referral to a sleep specialist is recommended. One panellist dissented, arguing that the treatment of CSA or mixed SDB using oxygen or pharmacotherapy remains controversial. The medical treatment of any associated CVD in patients with CSA or mixed SDB should also be optimised to improve outcomes.
Limitations
As a result of the obesity epidemic, the prevalence of OSA in Asia has increased in recent decades. However, the awareness of OSA in patients in Asia is low.51 These consensus recommendations aim to guide practising cardiologists and internal medicine specialists practicing cardiology on the management of patients with CVD with regard to OSA screening, diagnosis treatment and referral in the Asia-Pacific region. The 11 recommendations presented in this paper aim to guide clinicians based on the most up-to-date evidence. However, given the varied clinical situations and healthcare resources present in the region, these recommendations should not replace clinical judgement.
Conclusion
Management of patients with CVD and OSA should be individualised and should consider the patient’s symptoms, clinical characteristics and comorbidities, as well as patients’ and caregivers’ concerns and preferences. Clinicians should also be aware of the challenges that may limit the applicability of these consensus recommendations, such as limited access to specific interventions and technologies, limited availability of resources, accepted local standards of care, cultural factors and individualised expertise in OSA management.